
Disseminated Gonorrhea or Neisseria Gonorrhoeae. Disseminated gonococcal infection (DGI)
Many of my patients with Gonorrhea( pus per urethra) present with rash , some have joint pain (Gonococcal arthritis)
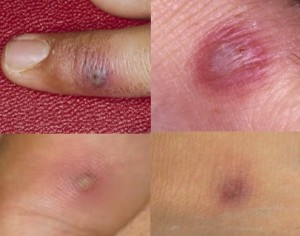
(DGI) follows untreated mucosal infection in about 0.5-3 per- cent of patients. Skin lesions are the most common manifestation of DGI and occur in 50-70 percent of patients. The eruption typically appears during the first day of symptoms and may recur with each bout of fever. The skin lesions associated with DGI begin as tiny red papules or petechiae 1-5 mm in diameter, many of which evolve rapidly through vesicular or pustular stages to develop a gray necrotic center, often on a hemorrhagic base. Papules, bullae, pustules, and hemorrhagic lesions may all be present simultaneously. The lesions tend to be scanty but widely distributed. The distal portions of the extremities are most commonly involved, with sparing of the scalp, face, trunk, and oral mucous membranes. Histologic examination will reveal local vasculitis, fibrin deposition, necro- sis, and neutrophil infiltration. Gram-stained smears of material from skin lesions infrequently reveal organisms, although most smears are positive for gonococci when examined by immunofluorescence techniques. Circulating immune complexes may play a role in the pathogenesis.